In honor of International Drug Checking Day on March 31, 2017, Erowid is giving away coupon codes for free EcstasyData analyses and Erowid schwag.
Submit a qualifying experience report to the Experience Vaults before the end of April 2017 and be eligible for this giveaway. Describe your experience doing drug checking (either personally, or as a harm-reduction worker) or a situation that needed drug checking, or write about an experience taking a psychoactive drug of any kind. Winning submissions will demonstrate risk minimization principles. Description of utilization of drug checking preferred but not required to enter.
What you can win:
HipLogo Shirt
1st Prize – Editors’ Choice: Best submission will receive a free EcstasyData GC/MS test, Erowid HipLogo t-shirt, and Erowid canvas tote bag.
2nd Prize – Triagers’ Choice: Erowid volunteers will select the second winner to receive a free EcstasyData GC/MS test & Erowid HipLogo t-shirt.
3rd Prize – 1 per 25 qualifying submissions will randomly be selected to receive a free EcstasyData test code and a free Erowid HipLogo t-shirt.
EcstasyData test results include reagent photos as well as GC/MS identification of substances in the sample, but not the quantity of substances present (as allowed by US law).
The more qualifying submissions we receive in honor of International Day of Drug Checking, the more free testing codes we’ll give away. Winners will be contacted in May.
To be eligible:
Include “IDODC” (or IDCD works, too) in the report’s first line.
Include your email address in the appropriate field of the report submission form. Email addresses are not shared, are protected on Erowid’s servers, and will only be used to contact report authors about their submission.
Original submissions previously self-published or posted elsewhere online are eligible to win but must meet all other criteria. Please don’t plagiarize.
Erowid staff and volunteers of Erowid are not eligible.
In May after winners have been contacted, Erowid will announce how many submissions were received and how many prizes were given away.
Thank you for participating in International Drug Checking Day!
On January 20th, The Sydney Morning Herald published “Pill testing sounds like a great idea, but there’s a catch”, by forensic toxicologist Andrew Leibie, who reasoned that field testing is not very helpful, and might be worse than nothing. Leibie seemed to both not understand what he was talking about, and to ignore some of the key benefits of having on-site testing at events where illegal drugs might be consumed.
A few days later, Monica Barratt responded with a critique of Leibie’s flawed article. In “Pill testing is still a great idea, if we use the right equipment”, she took Leibie to task for his assembling a series of partially true statements into a confused and ultimately wrong argument.
I have some points I want to repeat and add, since this is something we care (and know) a lot about.
Engaging Users
First, let me just be clear about a critical function of on-site drug checking: engaging people is the most important step in harm reduction. Once people start thinking about and taking steps to mitigate the risks they expose themselves to, everything else is gravy. Leibie argues from confused and incomplete data that on-site pill testing is ineffective and may be worse than nothing. For example, he strangely compares rates of deaths from new psychoactive substances (NPS) in the UK to those in Australia, and uses the comparison to imply on-site pill testing doesn’t reduce harm.
Reducing Harm, Not Eliminating Harm
Second, to paraphrase one of our colleagues: “It’s not about eliminating harm, it’s about reducing it. Taking drugs, like every other activity in life, is never ‘safe’.”
On-Site Testing Is Not Just Done with Reagents
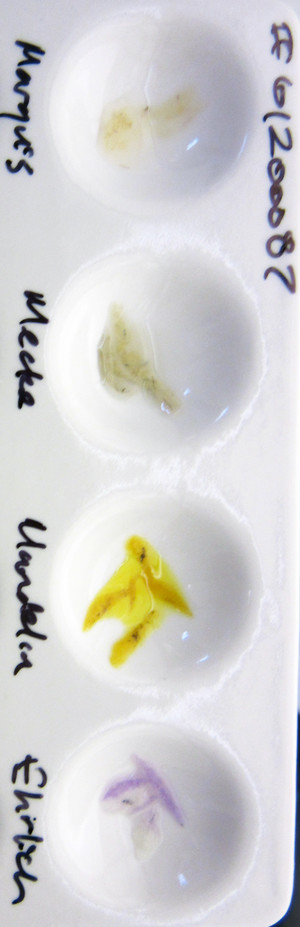
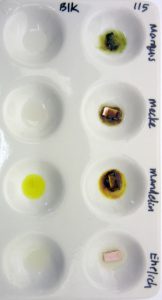
Third, it’s key to understand that on-site drug checking, what we might call “field testing”, can span a wide range of different methods. The most common are reagent tests like Marquis, Mecke, Simons, etc. These are simple “rule-in / rule-out” tests. Liquids are dropped onto scrapings or dust from a sample and may or may not change color. To a person experienced in the use of reagents tests, the color and timing can tell a lot about a sample. What reagents tests can’t do is positively identify anything.
They rule chemicals in and rule them out. If a pill shaving has Marquis reagent applied to it and there is no color change, then it is almost guaranteed that the sample contains, at most, a tiny trace of MDMA. MDMA is ruled out. If the sample + Marquis changes to a dark purple-then-brown color, then MDMA is “ruled in”. This means simply that the reagent reaction is consistent with MDMA and not, as some believe (including some law enforcement personnel trained to use these field tests), that the sample has been shown conclusively to contain MDMA.
There are an unknowable number of different reasons why the Marquis + sample could change color to the typical dark purple/blue/brown. The presence of certain dyes in a sample, temperature, a reagent past its “best by” date, opioids, and potentially yet-unknown other chemicals can produce that color when a sample comes in contact with Marquis. All we can say is, if there’s a color change consistent with how MDMA would react, MDMA is ruled in as a possibility.
Better Guesses are Better
Or, in Leibie’s mischaracterization, “the proposed colourimetric on-site pill test kits provide results that are little more accurate than ‘best guesses’.”
There are a couple things wrong with the wording of Leibie’s assessment of colorimetric field reagent testing. First, “best guess” is obviously better than a bad guess. Second, in every case I can think of, the use of a reagent test would be preferable to not using a reagent test at all. The color changes are informative but not final proof. They are definitely more relevant than a “best guess” made in the absence of any drug checking methodology.
But back to the bigger error: Leibie seems to conflate on-site pill checking with field reagent testing and then draw conclusions that are out of step with current trends. A growing number of groups are using much more interesting and accurate methods to analyze and identify drugs on location at events and festivals.
European On-Site Analysis
Groups like Austria’s CheckIt!, one of the partners in our EcstasyData lab analysis project, don’t “guess”. They run a mobile HPLC-MS unit, optimized to function reliably in party settings, and use it on-site at events to do accurate identification and quantification.
Energy Control in Spain has developed procedures for using Thin Layer Chromatography (TLC) on-site, in hot and dusty tents at mega festivals. Their methodology and expertise make it possible to not only identify drugs but to get approximate quantification as well.
There are groups using mobile FTIR (Fourier transform infrared spectroscopy). FTIR has been around a long time, although as an on-site drug checking method it’s very new. FTIR is definitely capable of more than a “guess”. FTIR has a long history as a lab technique, returns results rapidly, and involves equipment small enough to potentially be workable for mobile on-site setups. FTIR can be used to positively identify chemicals and is considered a proper forensic lab method for identifying street drugs.
Near Future: Cheap Portable Spectroscopy
The utility of portable infrared or Raman spectroscopy in on-site drug checking is on the near horizon. Raman, IR, UV, and other absorption or back-scatter analytical technologies work by shooting a laser source at a sample and then reading the patterns of reflected or transmitted light and comparing that against a database of known patterns. In the next ten years, it is likely that the costs of these portable devices could drop below $500 per unit, and the databases of patterns could be extensive. Not quite ready for real world use, but… not too far away either.
On-Site Drug Checking Blocked, Banned, & Political
The primary reason these lab-grade testing methods aren’t more widespread is that the politics of drug checking are super horrid. There are critics, like Leibie, who are just confused about the usefulness and harm reduction aspects, but the much bigger problem is the world governments dominated by prohibitionist thinking. Prohibitionists actually argue that it is a bad idea to “make drug use safer” and provide “quality control for the black market”. In this very common paradigm, the goal is to make illegal drug use as physically risky as possible rather than trying to reduce the potential damage done to people.
From my perspective that’s wholly unethical and policies based on pretending people will never take MDMA and other psychoactives are not only delusional, they are mean-spirited and unjust. But that’s the world we live in.
In most countries, harm reduction work is hamstrung by the fact that it is illegal (as in go to jail) to provide accurate drug checking. It is also disallowed because event producers do not want to be perceived as “pro-drug” or possibly be held accountable for drug sales or use at their events if they’ve acknowledged that it occurs. Inviting a harm reduction team with a bunch of equipment to operate at a party is de facto condoning illegal drug use, or so goes the thinking.
The Real World: Field Reagents Better than Nothing
So, despite the viable options for offering high-quality analysis at large events, what we are often left with is young harm reduction workers equipped with small bottles of field reagents such as Marquis. Reagent tests don’t cost very much, they are affordable enough for it to be OK if they’re seized or destroyed by law enforcement, and the number one purpose for using them is still served: Engaging with people about the fact that there are risks to taking illegal drugs, that one can have a rational relationship to those risks, and the worst and most likely of those risks can be reduced with sufficient knowledge, some foresight, some help, and a little care.
Now, on to an examination of other weaknesses in Leibie’s piece:
MDMA Is Not “Often Fatal”
Leibie statement: “High doses of MDMA and methamphetamine are often fatal by themselves.”
Risks from high dose MDMA tablets are explicitly acknowledged through social media marketing methods, such as Global Drug Survey and Mixmag’s public health message, “Don’t Be Daft / Start with Half” (UK).
That sentence is deceptive because of the word “often”. Water is a deadly poison. A high dose of water is often fatal by itself. Aspirin is a deadly poison. A high (enough) dose of aspirin is often fatal by itself. Leibie properly points out that MDMA and meth, even when they are of known quality and quantity, are not totally safe. And there are cases of people doing reasonable doses and still dying. But those cases are extremely rare. There is little evidence that people frequently die from taking MDMA or methamphetamine that is higher in potency than they expected.
Some tablets sold in Europe contain over 200mg of MDMA, a startlingly high dose. A small woman taking that amount of MDMA could be taking a serious risk, but the chances of her dying because on-site pill checking failed to give her clear quantitative information are nearly zero. It is very likely, in fact, that if the woman in this scenario visited a harm reduction table and asked about the tablet she was thinking of taking, she would have been immediately informed that it was a strong tablet. The information that drug checking harm reduction workers provide is not limited to whether a reagent test color change is consistent with MDMA. They provide a lot of useful info and harm reduction suggestions. So, Leibie’s point, as stated, is faulty.
On-Site Testing Is Helpful Even with New Psychoactive Substances
Leibie statement: “The greatest concern however, is that on-site tests cannot detect new designer drugs on the market, such as flakka, liquid acid or NBOMe compounds.”
Sample of LSD dropped on blotter tested with Ehrlich reagent turns purple.NBOMe Results. NBOMes respond differently than LSD to field reagents
(Forget for a moment that the way the sentence is worded implies acid is a “new designer drug”…) This statement is misguided because of the inappropriate conflation of “on-site” with colorimetric field reagent tests. It’s also inaccurate because the NBOMe compounds do change color and can be ruled in or out even at very low doses. LSD (acid) is also detectable using field tests. The Ehrlich reagent turns purple in the presence of LSD. This sample of liquid LSD (far right) was dropped onto paper towel and the field tests did a fine job of showing the presence of LSD.
Leibie statement: “Unfortunately, these dangerous compounds frequently are mixed with more familiar drugs, such as ecstasy, speed or ice, requiring highly advanced scientific analysis to be detected.”
This statement underscores the author’s lack of awareness that “advanced scientific analysis” is a practical option for on-site testing, if only it weren’t disallowed in most places. It also suggests a weak understanding of the field reagents he’s so strongly arguing against. Reagent field tests can rule in or rule out two of the three most “dangerous” drugs that he lists, the NBOMes and LSD (acid). For alpha-PVP (referred to as “flakka” here), he is right that it does not change color with the standard Marquis, Mecke, or Mandelin reagents. What a tremendous teaching opportunity for harm reduction workers to talk about adulterated drugs and the uncertainty of field tests (they can even point people to illustrative examples from EcstasyData, where we have reagent results side by side with the GC/MS lab findings). It seems Mr. Leibie is arguing against having those educational opportunities at large festivals.
And, while there are plenty of examples of NPS substituted for or adulterating more familiar drugs, the accuracy of the claim that this is a “frequent” occurrence is moot, since, just as the author points out that there are “no quality or consistency guarantees” for illicit drugs, there are also no representative sets of data about analyses of illicit drug samples available for public scrutiny (except maybe in the Netherlands). Law enforcement groups may analyze samples of seized drugs, but results are not typically shared with the public.
No Evidence that On-Site Testing Worsens Risks
Leibie statement: “Countries that have gone down the pill testing route do not provide any comfort that this approach works.”
Leibie makes several errors in the text he uses to support this statement. First, there is nothing like a valid apples-to-apples comparison between the different countries. Australia has a unique illegal drug market that is distinct from the UK’s. The Australian government runs one of the tightest customs operations in the world, in the confines of its own island continent, impacting Australia’s drug market much differently than the European-influenced UK. It is unclear why Leibie would feel qualified to offer a comparison of the effectiveness of unspecified relative amounts of harm reduction efforts in unspecified numbers of events with an unknown number of participants. It’s just weird. His statement qualifies as “most likely wrong”. The Netherlands are one of the only countries that has anything like a proper “pill testing route” with their DIMS project. And they don’t allow on-site lab gear at big events run by harm reduction workers.
False Sense of Security: A Real Problem
Leibie statement: “They also potentially leave consumers with a false sense of security that the party drugs they buy may be safe. It could be a deadly assumption.”
I think this is perhaps the most helpful statement in Leibie’s article. There is no question that many people misunderstand the risks of the drugs they are taking. Moreover, inexperienced use of field reagents can provide a false sense of security. People sometimes confuse lower risk with “safe”, or mistake harm reduction for harm elimination.
And it’s true that, sadly, sometimes people die after taking pharmaceuticals or recreational drugs in reasonable ways.
On-Site Testing Makes the World Better, Not Worse
Although the prominence of Leibie’s article offered a great opportunity to discuss the pros and cons of on-site testing, particularly the entirely relevant strengths and weaknesses of reagent testing, this opportunity was missed.
The author showed little knowledge of the specific area of music event or festival drug-checking. Performing tests at hot, dusty, remote events, with bass vibrations and the complexity of imaginative combinations of substances will always present challenges, but the experts running these services do tend to be well aware of these limitations.
The harm reduction projects that have been set up around the world are working within the parameters of government policies that seem at times to obstruct their efforts to serve the interest of public health. Despite all these conditions, and shoestring budgets, these groups are connecting people with specialist advice, mentors and peer support to ensure that on-site drug checking makes the world better, not worse.
Executive Summary: Different labs use different standards for reporting percentage purity assessments and also for mass when doing quantitative measurements for psychoactive drugs like MDMA. One lab’s 84% might be another lab’s 100%. This also means one lab’s 84 mg might be another lab’s 100 mg.
The publication of this article did not reveal a lot that we didn’t already know, but has brought into focus a heated argument that has been ongoing in public and private discussion forums about analytical methodologies for on-site and lab drug analysis.
What does it mean when a lab reports that a powder is 100% pure MDMA? What does it mean when a lab reports that a tablet contains 100 mg of MDMA?
The reason for writing about this is that there are no simple answers to those questions, though it seems like there should be.
Some online vendors of research chemicals have stated that various labs’ purity results in the 75-85% range mean that the sample was really “100% pure”, because of different ways of handling the mass of the sort-of-attached non-psychoactive salt anion. An anion is a negatively charged counter-ion that balances the positively charged, nitrogen-bearing drug molecule. When freebases are turned into salts, an anion is added.
The main case and the one that’s relatively easy to talk about is MDMA. MDMA is normally produced and distributed as MDMA hydrochloride (HCl), which is MDMA in a solution that has been converted to a crystalline form—-a “salt”-—by bubbling hydrochloric acid gas through the liquid. This causes the MDMA to turn insoluble in the solvent, precipitating out as MDMA HCl crystals. There are other possible salt forms of MDMA, but this is the “table salt” (most common salt form) of ecstasy/molly.
In fact, normal table salt or culinary salt is usually considered Sodium Chloride, or NaCl. We’re virtually swimming in tiny amounts of acids and salts in our normal environments. Remember your protective eyewear!
In addition to chloride salts like HCl, there are numerous anion salts possible, such as sulfide, fluoride, and bromide. For some psychoactive chemicals, the specific salt form can make a big difference in determining a dose. Mescaline has been distributed historically as Mescaline hydrochloride, Mescaline sulfate, Mescaline citrate, and Mescaline acetate. All of these have slightly different mass ratios between the base mescaline molecule and the portion that is the partially-bound anion. One could theoretically get 25% more or less mescaline, from a consistently weighed amount, depending on which salt form is involved.
This can be super complicated and technical and I doubt anyone is reading this who doesn’t get the basic premise. But there are technical issues like having some salt anions that bind two-to-one or one-to-two in crystalline forms. See What is the molecular weight of LSD tartrate? and many, many other discussions for crazy-making levels of detail.
As lab testing using GC/MS, HPLC, and FTIR has become more available and more projects are publishing their data and providing harm reduction information to individuals on the basis of their findings, it becomes increasingly important for more people to understand basic elements of some of the technical issues involved.
When this question of MDMA mass came up again this week, we asked the authors of the paper and the folks who work at Trimbos the following:
It has been suggested that DIMS might be using MDMA Freebase as the basis for mass and purity calculations, rather than salt masses, such as MDMA HCl. It is not described in any of your papers that I can find, but perhaps these questions will simplify the issue:
1) If DIMS received a powder sample of material that contained only MDMA HCl and nothing else, what would the reported purity be? 100%?
2) If DIMS received a tablet sample that contained 100 mg of MDMA HCl and 200 mg of lactose and inactive binders, what would the reported amount of MDMA be in that tablet? 100 mg? or would that qualify under your reporting rules as 84 mg of MDMA (freebase)?
And we got a very clear answer from the excellent Dr. Tibor Brunt:
“Indeed we use freebase as analysis standard. That actually means that if we report 100 mg MDMA in a pill, it is 119 mg in MDMA HCl. Our lab has always left out the salt component of psychoactive substances, since this component is not psychoactive. And if we’d receive a powder with 100% MDMA HCl this would be 84% maximum purity like you said.”
The reason they would define pure MDMA HCl crystal as only 84% pure is a little technical, but suffice to say it is not the only way to report an analytical result.
The reason that an expert group like Trimbos would decide to report masses this way is to normalize all their information across all salt forms of MDMA. I imagine, though I don’t know, it could be related to different types of quantitative methodologies that they have been working with for a long time.
So, dear drug geek reader, the question is not whether this issue is real, but, exactly what methodology and reporting measures are used by the analytical group you’re working with.
Energy Control of Spain, on the other hand, answered that they use MDMA HCl as their mass standard. They answered the questions clearly:
1) Our results directly provide the result of the salt of the substance, as
we’re using a salt as a reference standard. This means that the purity of a
sample with only MDMA HCl could be 100%.
2) Therefore, a tablet with 100mg of MDMA. HCl would be reported as 100mg
of MDMA.
SaferParty and the cluster of groups in Switzerland that do work around that brand are very clear in all of their caution and warning publications that they are using MDMA HCl as their basis. For instance, “120 mg MDMA * HCl können zu viel sein”.
On Jan 30, 2017, they followed up with a long detailed answer to our questions.
Dear Earth,
Here the answer from our lab, i hope this clears things up:
As a reference standards-producing laboratory we’ve got most of our standards as solids in our hands, e.g. (water-free) salts. This is in contrast from what you get most times when buying solutions of reference standards from other companies (e.g. Cerilliant etc.). They usually sell the free base as a solution. Due to that, we are using mostly salts for calibrations. The second reason for that is, most of the time we are obtaining samples in salt forms for analysis (e.g. cocaine, heroine, MDMA, amphetamine, methamphetamine and other phenethylamines etc.); though we do not determine what kind of salt the sample consists of (e.g. hydrochloride, sulfate, acetate etc.).
We have had quite good experiences with this so far, as the sum of e.g. mixtures of amphetamine-coffeine-containing samples, when otherwise pure, reach 100% in sum when calculated with amphetamine hydrochloride. When exceeded 100% one may assume it contains a certain amount or all as free base. When the results are displayed as free base one can calculate any possible salt form. We think, according to the black market products here in Switzerland, it makes sense to give the results calculated for the hydrochloride salts, but for comparison with other labs/other countries the use of free base content would be the only value to make sense. Nevertheless, our results can easily be recalculated to the free base content, at least when knowing the type of compound we applied for calibrations/calculations.
We see it from the way that most dosage recommendations for a psychoactive compound to be taken orally or by snorting are given in the salt form (if possible), so this substantiates the indication as salt. With DMT as an example, we indicate the free base as content.
A short question the relatives the senses of indicating “purity” or “content”:
When having a chemically pure amphetamine sulfate (e.g. 100% Amphetamine sulfate”), its content of amphetamine free base is 73.4%. When having chemically pure amphetamine hydrochloride (e.g. 100% amphetamine hydrochloride), its content of amphetamine free base is 78.8%. When only seeing these numbers, which would you judge to be more pure? The lay would say it to be the second, but chemically both salt forms are chemically absolutely pure (100%).
A problem that comes in is, when having, e.g., a chemically impure amphetamine hydrochloride and reaching a displayed content of 73% amphetamine free base, one may imagine this to be a nearly chemically pure sulfate (close to the maximum content of 73.4%), but in fact it is a rather impure hydrochloride (73% out of a maximum content of 78.8%). As long as one does not determine the counterion (salt) this remains problematic.
When calibrating and calculating with salts, a measured sample consisting of free base would yield a result above 100%.
Each calibration/calculation has its own advantages, be it the use of free base, hydrochlorides, or hydrochlorides monohydrate, etc.
Let’s go to your questions:
“1) If SaferParty received a powder sample of material that contained only MDMA HCl and nothing else, what would the reported purity be? 100% ?”
As we used waterfree MDMA*HCl for calibration, we would report 100% content. As most of the samples measured here are on hand as the monohydrate (MDMA*HCl*H2O), the measured content mostly lies around a maximum of 93%.
“2) If SaferParty received a tablet sample that contained 100mg of MDMA HCl and 200mg of lactose and inactive binders, what would the reported amount of MDMA be in that tablet? 100mg ? or would that qualify under your reporting rules as 84mg of MDMA (freebase)?”
Our reported content would be 100mg MDMA*HCl.
The Loop offers analysis at music events in the UK to improve safety for partygoers and facilitate care by medical staff. When they report quantitative results for MDMA, they answered our questions as follows:
1. 100% purity
2. 100mg of MDMA (since the HCl salt is ubiquitous and service users
simply call MDMA.HCl “MDMA” we do not complicate the information they are
already getting with a description of why we are calling it something
different).
CheckIt! Austria very generously took their question to their technical staff and verified their answer before getting back to us:
Our chief chemist just got back to regarding your question.
We use MDMA.HCl to prepare our standards for quantitative measurements. So if we would receive sample solely consisting of MDMA.HCl, the result would be 100%. Quantitative MDMA results in tablets are also reported as HCl. So if a tablet contains 100mg MDMA.HCl and let’s say 100 mg alpha-Lactose monohydrate we would report 100mg MDMA content.
One of the thing that stands out to us as problematic when encouraging our species and societies to have balanced views about psychoactives, and is part of the reason that the public policy is a rolling global disaster, is that most data published about harms is selectively chosen for greatest impact.
Some authors published a complete summary of all “all cases presenting at the emergency department (ED) of the University Hospital of Basel, Switzerland, between October 2014 and September 2015 with acute toxicity due to self-reported recreational drug use or with symptoms/signs consistent with acute toxicity.”
It is unfortunately, from our view, that they did not also then include in their analysis presentations related to pharmaceutical drugs, but this is a great start.
Their summary speaks for itself, but imagine a world where all major hospitals published anonymized case data and we could get this type of summary every year?! It’s just too much to imagine that we might base education, expectation, and public policy on real world understandings of that relative magnitude of harms, rather than the most recent scary news story or the grieving parents of a tragic fatality.
Their paper is not as extensive as it could be and we’d really like to see a matrix table of what drugs were found combined with other drugs. Also, the authors did not have the ability to detect or identify new synthetic cannabinoid receptor agonists.
About a third of the cases were “related to” cocaine and a third “related to” cannabis. The next most common self-reported substances were heroin, benzodiazepines, MDMA, amphetamine/meth, unknown, and then opioids (excluding heroin and methadone).
Perhaps the biggest question is how good their detection / analysis is. Would they be able to detect MXE or deschloroketamine or other really new substances if they had been present?
Background
Although the recreational use of psychoactive substances is common there is only limited systematic collection of data on acute drug toxicity or hospital presentations, in particular regarding novel psychoactive substances (NPS) that have emerged on the illicit market in the last years.
Methods
We included all cases presenting at the emergency department (ED) of the University Hospital of Basel, Switzerland, between October 2014 and September 2015 with acute toxicity due to self-reported recreational drug use or with symptoms/signs consistent with acute toxicity. Intoxications were confirmed using immunoassays and LC-MS/MS, detecting also novel psychoactive substances.
Results
Among the 50’624 attendances at the ED, 210 were directly related to acute toxicity of recreational drugs. The mean patient age was 33 years and 73 % were male. Analytical drug confirmation was available in 136 cases. Most presentations were reportedly related to cocaine (33 %), cannabis (32 %), and heroin (14 %). The most commonly analytically detected substances were cannabis (33 %), cocaine (27 %), and opioids excluding methadone (19 %). There were only two NPS cases; a severe intoxication with paramethoxymethamphetamine (PMMA) in combination with other substances and an intoxication of minor severity with 2,5-dimethoxy-4-propylphenethylamine (2C-P). The most frequent symptoms were tachycardia (28 %), anxiety (23 %), nausea or vomiting (18 %), and agitation (17 %). Severe complications included two fatalities, two acute myocardial infarctions, seizures (13 cases), and psychosis (six cases). Most patients (76 %) were discharged home, 10 % were admitted to intensive care, and 2 % were referred to psychiatric care.
Conclusion
Most medical problems related to illicit drugs concerned cocaine and cannabis and mainly included sympathomimetic toxicity and/or psychiatric disorders confirming data from the prior year. Importantly, despite the dramatic increase in various NPS being detected in the last years, these substances were infrequently associated with ED presentations compared with classic recreational drugs.
The Dutch drug testing program does not allow for mailed-in samples (folks have to bring them in person) and they never publish individual results publicly, nor do they publish summaries contemporaneously. Only warnings about “dangerous drugs” are published soon after a sample’s analysis. Despite these limitations, the Nederlands Ministry of Health’s Drug Information and Monitoring System (DIMS) is one of the best testing projects in the world.
The DIMS Annual Report for 2015 says the project analyzed nearly 12,000 samples in 2015 alone.
Their program works by individuals bringing samples in to one of the approved locations, in person. In some cases (like with pharmaceutical tablets) the drug identification is provided immediately. In other cases (they do not specify frequency) they send the sample in to a lab and the individual who brought in the sample is given a unique code, which they can use to call back in a week and get the analysis result.
They had an amazing 28 physical locations in 2015 in a country the size of Ohio. Free testing, in every major city and some minor ones. NOt more than an hour’s transit away. There’s nothing else like it.
Some highlights (thanks roi):
57% of the ecstasy pills they tested contained over 140 mg MDMA
The highest dose in an ecstasy tablet was 293 mg MDMA
Average cocaine purity was 64%
Average amphetamine purity was 46%
4-FA (4-fluoroamphetamine) was the most tested “research chemical”
LSD blotter contained an average of 74 ug LSD
27% of samples sold as “LSD” didn’t contain LSD
11% of ketamine samples contained MXE or deschloroketamine
Average MDMA dose in tablets has greatly increased over the last 10 years
Amphetamine and cocaine purity slightly increased over the last 10 years